This from School finance 101:
Arne Duncan has one whopper of an interview available here: http://www.msnbc.com/andrea-mitchell-reports/watch/better-preparing-our-nations-educators-237066307522
Related to his new push to evaluate teacher preparation programs using student outcome data: http://schoolfinance101.wordpress.com/2014/04/25/arne-ology-the-bad-incentives-of-evaluating-teacher-prep-with-student-outcome-data/
And his Whitehouse press release can be found here: http://www.whitehouse.gov/the-press-office/2014/04/25/fact-sheet-taking-action-improve-teacher-preparation
Now, there’s a whole lot to chew on here, but let me focus on one of the more absurd hypocrisies in all of this.
First, Duncan seems to think the world of medical education without apparently having the first clue about how any of it actually works. In his view, it’s really just a matter of intensive clinical training (no academic prerequisites required) and competitive wages (a reasonable, though shallowly articulated argument).
Second, Duncan also seems to think that a major part of the solution for Ed Schools can be found in entrepreneurial startups like Relay Graduate School of Education. The Whitehouse press release proclaims:
Relay Graduate School of Education, founded by three charter management organizations, measures and holds itself accountable for both program graduate and employer satisfaction, and requires that teachers meet high goals for student learning growth before they can complete their degrees. There is promise that this approach translates into classroom results as K-12 students of Relay teachers grew 1.3 years in reading performance in one year.Now, I’ll set aside for the moment that the student outcome metrics proposed for use in evaluating ed schools create the same bad incentives (and unproven benefits) that the feds have imposed for evaluating physicians and hospitals.
Let’s instead consider the model of the future – one which blends Arne Duncan’s otherwise entirely inconsistent models of training. I give you:
The Relay Medical College and North Star Community Hospital
Here’s how it all works. Deep in the heart of some depressed urban core where families and their children suffer disproportionate obesity, asthma and other chronic health conditions, where few healthy neighborhood groceries exist, but plenty of fast food joints are available, sits the newly minted North Star Community Hospital.
It all starts here. NSCH is a new kind of hospital that does not require any of its staff to actually hold medical degrees, any form of board certification or nursing credential, or even special technician degrees to operate medical equipment or handle medications. Rather, NSCH recruits bright young undergrads from top liberal arts colleges, with liberal arts majors, and puts them through an intense 5 week training program where they learn to berate and belittle minority families and children and shame them into eating more greens and fiber. Where they learn to demean them into working out – walking the treadmill, etc. It’s rather like an episode of the Biggest Loser. And the Hospital is modeled on the premise that if it can simply engage enough of the community members in its bootcamp style wellness program, delivered by these fresh young faces, they can substantively alter the quality of life in the urban core.
There is indeed some truth to the argument. Getting more community members to eat healthier and exercise will improve their health stats, including morbidity and mortality measures commonly used in Hospital rating systems. In fact, over time, this Hospital, which provides no actual medical diagnosis and treatment does produce annual reports that show astoundingly good outcome measures for community members who complete their program.
These great outcome measures generate headlines from the local news writers who fail to explore more deeply what they mean (Yes Star Ledger editorial board, that’s you!). NCSH becomes such a darling of the media and politicians that they are granted authority to start their own medical school to replicate their “successes.” And they are granted the authority to run a medical school where medical training need not even be provided by individuals with medical training!
Rather, they will grant medical degrees to their own incoming staff based on their own experiences with healthcare awesomeness. That’s right, individuals who themselves had little or no basic science or actual supervised clinical training in actual medicine, but have 3 to 5 years of experience in medical awesomeness in this start-up (pseudo) Hospital will grant medical degrees – to their own incoming peers!
Acknowledging the brilliance of this new model, US Dept of Health officials established a new rating system for all medical colleges whereby they must show that graduates of their programs reduce patient morbidity and mortality. RMC and NCSH continue to lead the nation, despite providing no actual medical interventions, but sticking to their plan of tough love, no excuses wellness training.
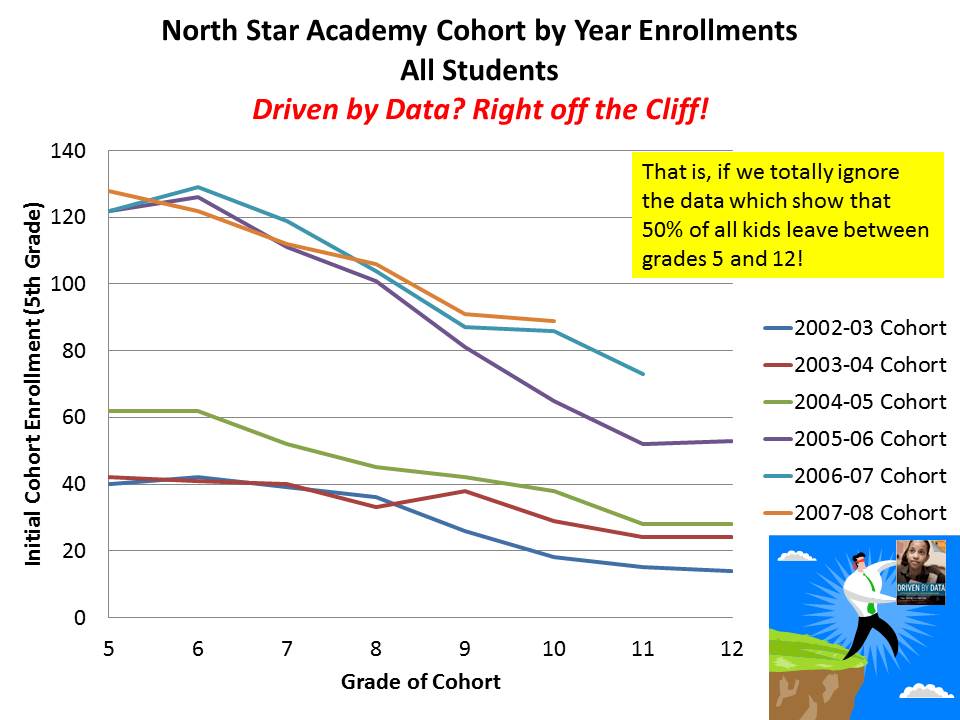
But, one day, it comes to light that while approximately 50 community members per year who succeeded in NCSH program and did in fact experience improved quality of life, there had been over 150 entrants to the program each year (like this). In fact, most failed. Some simply weren’t up for the daily berating inflicted on them by NCSH staff. Some had other chronic health ailments and were told by NCSH staff to suck it up, get in line (literally, in line, step left only when told) or leave.
It became clear that patients with diabetes and heart conditions need not apply. None of the staff employed at NCSH had training in cardiology or for that matter any CPR or basic life support skills. That stuff really didn’t matter to them and they sure as heck weren’t going to stand for someone keeling over on the treadmill, and lowering the NCSH mortality stats.
Sadly, by this point in time RMC and NCSH had become such a touted model that the real urban hospitals had all been closed. Further, there were few if any incentives for real medical colleges to train physicians to work in the urban core, where the traditional medical model had now been fully replaced by the RMC/NCSH model. They certainly couldn’t match the stats that NCSH was posting if they chose to serve patients who actually had chronic health conditions, or were non-compliant patients.
And those 100 dropouts of the NCSH program from each cohort, those with diabetes, heart disease and other health conditions not so easily mediated with a good shout down, were simply out luck. Actual community morbidity and mortality stats skyrocketed. But alas, no one was left to care.
Note:
Indeed, wellness is key to the provision of high quality healthcare in the urban core and elsewhere. But it is not a replacement. And yes, one can make an argument that the bootcamp program described above as NCSH legitimately helped to improve the health outcomes and perhaps even the overall quality of life for the 50 program completers, as does the reality TV show Biggest Loser.
One can certainly make the comparison to the benefits obtained by the 50% or so actual completers of the most no excusiness charter schools like North Star Academy in Newark, NJ. Those few students who do succeed and complete are likely better off academically than they might have otherwise been. But this by no means indicates that North Star Academy and Relay Graduate School of Education, or my hypothetical North Star Community Hospital and Relay Medical College are model programs for serving the public good. In fact, as pointed out here, assuming so, applying bogus easily manipulated and simply wrongheaded metrics to proclaim success, may in the end cause far more harm than good.
{kind=link}
No comments:
Post a Comment